 Thyroid nodules are growths in the thyroid. Thyroid nodules are very common and occur in up to 15 to 30% of the US population. Like most thyroid diseases, they are more common among women than men. In addition, the chance of having a thyroid nodule increases with age and by the time a woman is 60, there is a 60% chance that she will have a thyroid nodule. Although many thyroid nodules can be felt by the patient or by a doctor during physical examination, more and more nodules are being discovered incidentally during an imaging test (like carotid USG or CAT scan) being done for another reason.
Thyroid nodules are growths in the thyroid. Thyroid nodules are very common and occur in up to 15 to 30% of the US population. Like most thyroid diseases, they are more common among women than men. In addition, the chance of having a thyroid nodule increases with age and by the time a woman is 60, there is a 60% chance that she will have a thyroid nodule. Although many thyroid nodules can be felt by the patient or by a doctor during physical examination, more and more nodules are being discovered incidentally during an imaging test (like carotid USG or CAT scan) being done for another reason.
The most important questions to ask when a thyroid nodule is discovered are:
- is the patient hyperthyroid (i.e. do they have too much thyroid hormone in their body)? and
- is this a cancer?
Fortunately, most thyroid nodules are benign (i.e. not cancer) and non-functional (i.e. not causing hyperthyroidism). Only 5 to 10% of thyroid nodules will end up being cancer.
The Columbia Thyroid Center offers a special Thyroid Biopsy Clinic to provide single day evaluation of thyroid nodules.
Signs and Symptoms
Most thyroid nodules do not cause symptoms (i.e. they are asymptomatic). In fact, many patients will not know that they are there. If a nodule is hyperactive, patients may experience the signs and symptoms of hyperthyroidism.
Patients with large nodules may notice a palpable mass (i.e. a mass they can feel) or a visible mass (i.e. a mass they can see). Very large nodules may cause compressive symptoms which include difficulty swallowing, food or pills getting "stuck" when they swallow, and pressure or shortness of breath when lying flat. Patients with compressive symptoms, enlarged lymph nodes, hoarseness, and/or a rapidly growing nodule should seek medical evaluation right away.
Diagnosis and Treatment
When a thyroid nodule is discovered, a complete history and physical examination should be performed.
In particular, the doctor is looking for risk factors for cancer that include: a family history of thyroid cancer, a history of radiation exposure to the head, neck, and/or chest, age less than 20, age greater than 70, male gender, very hard nodules, enlarged lymph nodes, and/or hoarseness. After the history and physical exam, a TSH level should be checked to see if the patient is hyperthyroid. A lower than normal TSH may mean that the patient is hyperthyroid. If this is the case, then a radioactive iodine scan (RAI scan) should be done to determine if just the nodule is hyperactive or if it is the whole gland. Hyperactive areas will "light up" on RAI scan and are unlikely to be cancer and therefore do not require biopsy.
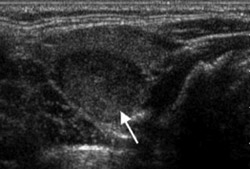
The next step in the work-up of a thyroid nodule is an USG of the neck. There is no radiation associated with an USG. An USG is the best test to look at the thyroid and will allow the doctor to see the size of the thyroid and specific features of the nodule(s) including: size, number of nodules, if there are calcifications (calcium deposits), echotexture (i.e. how bright or dark it looks on USG), borders, shape, and if it is solid or cystic (i.e. fluid-filled).
The best test to determine if a thyroid nodule is benign or cancer is a fine-needle aspiration biopsy (FNAB). In this test, a small needle (like the needles used for drawing blood) is placed into the nodule either by USG or feeling the nodule with the fingers. Cells are removed from the nodule into the needle (i.e. aspirated) and looked at under the microscope by a specially trained doctor called a cytologist. There are a number of different guidelines as to which nodules should be biopsied, but in general, nodules over 1 cm should be biopsied. If a patient has risk factors for thyroid cancer (especially a family history of thyroid cancer or exposure to radiation therapy) or suspicious findings on USG, then nodules over 0.5 cm should be biopsied. The FNAB may give one of 4 results:
Non-diagnostic: This means that not enough cells were removed to make a diagnosis. Even in the best of hands, this happens in 5 to 10% of FNAB. Typically the FNAB will be repeated. If the nodule grows, then a repeat biopsy will usually be performed. In certain cases, a patient may go straight to an operation to make a diagnosis, especially if the risk of cancer is high or if the patient has had two or more non-diagnostic FNAB in the past.
Benign: This means that there is a 97% chance that the nodule is not cancer. In most cases, patients with a benign biopsy are watched with an USG and physical exam 6 months later, and then at regularly scheduled times. A patient with a benign nodule may still have an operation if the nodule is large, causing symptoms, or cosmetically unappealing.
Malignant: This means that there is a 97% chance that the nodule is cancer, usually a papillary thyroid cancer. Much less commonly, the FNAB can show a medullary or anaplastic thyroid cancer. Sometimes the cytologist reports that the nodule is "suspicious for thyroid cancer" which means that there is an 80 to 90% chance of cancer, again usually papillary thyroid cancer. Most patients with a FNAB of cancer will have a total thyroidectomy (i.e. removal of the entire thyroid) with or without removal of certain lymph nodes.
Indeterminate: This category includes different readings like: follicular lesion, follicular neoplasm, Hurthle cell lesion, Hurthle cell neoplasm, and atypical cells or atypical lesions. This means that the cytologist cannot tell if the nodule is cancer, but the cells do not look normal. There is a 15 to 20% chance of having thyroid cancer with an indeterminate biopsy. Said another way, 1 out of 5 people with an indeterminate biopsy will have cancer. The only way to make a clear diagnosis of cancer or no cancer is to remove half or all of the thyroid and see if the cells in the nodule are invading (i.e. growing) outside of the nodule into the surrounding thyroid or outside of the thyroid.
Next Steps
If you are dealing with a thyroid issue, our team at the Columbia Thyroid Center is here to help. Call (212) 305-0444 or request an appointment online.