Guide to Pectus Excavatum
Pectus excavatum is a condition in which the chest wall is sunken in, creating a caved-in appearance.
Key Info
- Pectus excavatum is a relatively common congenital deformity.
- Severe cases of pectus excavatum can affect lung capacity, causing fatigue, shortness of breath, chest pain, and a fast heartbeat
- There are multiple corrective surgeries for pectus excavatum
 Pectus excavatum is a malformation of the chest wall in which several ribs and the sternum (breastbone), grow abnormally, resulting in a caved-in, or sunken appearance. It is a relatively common congenital deformity and occurs more often in males than in females. Approximately 40% of people with pectus excavatum have one or more family members with the defect.
Pectus excavatum is a malformation of the chest wall in which several ribs and the sternum (breastbone), grow abnormally, resulting in a caved-in, or sunken appearance. It is a relatively common congenital deformity and occurs more often in males than in females. Approximately 40% of people with pectus excavatum have one or more family members with the defect.
Often present at birth, the condition may also develop during puberty and can range from mild to severe. Although its causes are not completely understood, the condition is believed to arise from excessive growth of the cartilage connecting the ribs to the breastbone, which pulls the sternum inward.
Pectus excavatum can compromise lung and heart capacity, especially when the condition is severe, causing fatigue, shortness of breath, chest pain, and a fast heartbeat. In some cases, the proximity of the sternum and the pulmonary artery may cause a heart murmur. For ordinary everyday activities, a person with pectus excavatum may have no symptoms, but with rigorous exercise, symptoms often appear. Lung capacity may be curtailed because lungs are confined and cannot properly expand.
During exercise, a person diagnosed with pectus excavatum compensates by engaging the diaphragm in breathing in order to enable the lungs to expand more and obtain adequate oxygen and carbon dioxide exchange for the demands of the body. The additional energy utilized for breathing in this manner contributes to fatigue. Those with severe pectus excavatum often notice that they are incapable of similar levels of activity as their peers. This can be especially difficult for adolescents, who often withdraw from participating in sports or other high-stress physical activities.
 In addition to its more serious symptoms, pectus excavatum may have negative psychosocial effects in children and teenagers, who often experience self-consciousness and difficult peer interactions stemming from their appearance. Often activities that expose the chest are avoided.
In addition to its more serious symptoms, pectus excavatum may have negative psychosocial effects in children and teenagers, who often experience self-consciousness and difficult peer interactions stemming from their appearance. Often activities that expose the chest are avoided.
Multiple tools are used to diagnose pectus excavatum and gauge its extent, including:
- Visual examination of the chest
- Auscultation — analysis of sounds of the heart and chest to detect the condition's effect on heart and lung function
- Electrocardiogram (ECG, also called EKG)
- Echocardiogram (a noninvasive test that takes a picture of the heart with sound waves)
- Pulmonary function testing (breathing into a mouthpiece connected to an instrument that measures the amount of air breathed over a period of time)
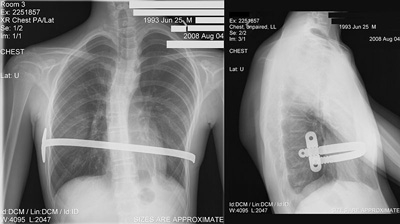
- Chest X-ray
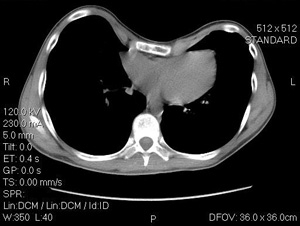
- CT-scan
- Haller Index: A measure of the extent of pectus excavatum by means of the CT scan. It is calculated by obtaining the ratio of the horizontal distance of the inside of the ribcage and the shortest distance between the vertebrae and sternum. A Haller Index of greater than 3.25 is generally considered severe (a normal Haller Index is 2.5).
Surgical Treatment
The ideal age for surgical treatment of pectus excavatum is between 12 and 18 years. The goal of surgery to correct a pectus excavatum defect is to improve breathing, posture, and cardiac function, in addition to giving the chest a normal appearance. This is typically accomplished by repositioning the breastbone. Surgical repair has excellent success rates and oftentimes, cardiovascular and lung function returns to near normal in the majority of cases.
Recovery after pectus excavatum repair varies depending on the person’s age and the amount of chest depression. After surgery, most people leave the hospital within 3 to 5 days and can return to school or work within two to three weeks. One must avoid vigorous exercise for the first month after surgery, and contact sports for three months after surgery.
Stories & Perspectives
Listen: Pectus Excavatum podcast from Columbia thoracic surgeon, Lyall. A. Gorenstein, MD
Nuss Procedure
 The minimally invasive Nuss procedure is performed with general anesthesia.
The minimally invasive Nuss procedure is performed with general anesthesia.
Performed using video-assisted thoracoscopic surgery or VATS, the Nuss procedure creates a horizontal passage underneath the sternum through two small incisions in the side of the chest. A separate, small incision enables the surgeon to view the inside of the chest with the thoracoscopic camera. A convex bar known as the Lorenz pectus bar is specially shaped to fit the individual’s anatomy, inserted through the passage, and then turned to push the sternum outward. The bar must remain in place for a minimum of three years while the chest contour re-forms to its new shape. The bar is removed as an outpatient procedure.
Many adults have undergone minimally invasive pectus repair with the Nuss procedure, which was originally developed for the repair of pectus excavatum in children. The results appear to be as good as with the modified Ravitch procedure (description follows below), which has been the traditional approach to repairing pectus excavatum in adults.
Modified Ravitch Repair
The procedure is performed under general anesthesia.
Utilizing a horizontal incision, the modified Ravitch technique involves removing small pieces of deformed chest cartilage and repositioning the protruding ribs and sternum. To support the repaired chest architecture, titanium bars are secured to the ribs and sternum.
Previously, the supports used to keep the sternum in place needed to be removed after several years. The bars currently used are secured to the chest wall in such a fashion that they can remain permanently in place, thereby avoiding the need for a second operation.
Next Steps
If you need help for a lung or chest issue, we’re here for you. Call (212) 305-3408 for existing patients, (212) 304-7535 for new patients, or request an appointment online to get started today.