Guide to Primary Hyperparathyroidism
Reviewed by the physicians of Columbia’s Parathyroid Surgery Team, October 2024
Primary hyperparathyroidism (PHP) is a disease in which one or more of the parathyroid glands are hyperactive and make too much parathyroid hormone (PTH). This constantly high PTH level causes an increase in blood calcium levels. PHP is the most common cause of high blood calcium levels in the general population and occurs in about 28 out of every 100,000 people. PHP is twice as common in women than in men and becomes more common as people get older with most cases occurring after the age of 45. The average age of patients with PHP is 65 years old. In 80% of cases, PHP is caused by a single hyperactive gland (single adenoma). However, PHP can be caused by 2 or 3 hyperactive glands (double or triple adenoma) in 10% of cases or 4 hyperactive glands (4 gland hyperplasia) in another 10% of cases. High calcium levels may be caused by other conditions such as cancer and too much calcium in the diet among other things, so it is important to work with experienced parathyroid experts to make the proper diagnosis.
Risk Factors
Although the causes of primary hyperparathyroidism (PHP) are not well understood, there are 2 main things which are known to put an individual at higher risk of developing the disease:
- a family history of parathyroid disease
- exposure to radiation
Family History
A family history of parathyroid disease carries the biggest risk for patients with first-degree relatives (mother, father, sister, brother), second-degree relatives (grandmother, grandfather, grandson, granddaughter), and/or multiple family members with parathyroid disease. PHP can be related to genetic syndromes called Multiple Endocrine Neoplasia type 1 (MEN 1) and Multiple Endocrine Neoplasia type 2 (MEN 2) Syndrome, and is usually the result of a specific genetic mutation in a part of the genome called the RET proto-oncogene. It is important that patients with a strong family history of PHP, as well as their families, be tested for this genetic abnormality (with a simple blood test) to see if they are at risk for developing the disease. Patients with MEN 1 Syndrome typically have pancreatic and pituitary tumors along with PHP. Patients with MEN 2 Syndrome typically have medullary thyroid cancer and pheochromocytoma (an adrenaline-producing tumor) in addition to PHP. See Medullary Thyroid Cancer » and See Pheochromocytoma ». While the majority of patients with MEN 1 Syndrome will develop PHP, only 33% of patients with MEN 2 Syndrome will develop PHP.
Radiation Exposure
In the 1960's it was discovered that exposure of the head and neck areas to radiation during treatment of benign diseases increases the risk of developing PHP. Since that time, this link has been found with exposure to significant doses of radiation from a variety of sources including:
- Medical Exposure In the first half of this century before antibiotics became available, radiation therapy was used to treat several benign diseases, such as acne, scalp ringworm, enlarged tonsils, enlarged thymus, enlarged lymph nodes in the neck as a result of tuberculosis, whooping cough, and keloid scars. In fact, over one million young Americans received x-ray treatments to the head or neck between 1920 and 1960. At the time, it was not known that the long-term effects of this radiation therapy to the head and neck area might cause PHP. When the association between radiation treatment and PHP and other health issues was established, the use of this type of therapy was largely stopped. However, some of the most common radiation exposures today are during critical radiation therapy for different forms of cancer such as breast cancer, lymphoma, and lung cancer, among others.
- Environmental Exposure In addition to radiation treatment, exposure to radiation as a result of nuclear weapons or nuclear plant accidents, such as that experienced by the survivors of Hiroshima, Nagasaki and Chernobyl, also increases the risk for developing PHP.
Of note, there have been NO long-term, high-quality studies that have demonstrated a link between diagnostic X-rays done for testing purposes and PHP. The doses of radiation associated with x-rays, CAT scans, and using devices such as cell phones, microwave ovens, etc. are too low to cause parathyroid disease. PHP may not develop for 30 to 50 years after the radiation exposure. People who were exposed to radiation are also more likely to develop thyroid nodules in general and should have any suspicious nodules evaluated. See Thyroid Nodules ».
Signs and Symptoms
 Over time, PHP damages almost every part of the body. Depending on how severe the disease is, PHP may cause virtually no symptoms or it may create severe, life-threatening symptoms. Doctors use the phrase "stones, bones, groans, psychic moans, and fatigue overtones" to remember that PHP can cause kidney stones, osteoporosis (i.e. weak bones), abdominal pain (i.e. pancreatitis, reflux disease), mental issues (i.e. depression, irritability, worsening concentration, worsening short-term memory, "brain fog"), and fatigue or low motivation levels among other things. When calcium levels become dangerously high (i.e. 13-15 range), patients may present in hypercalcemic crisis where their organs are failing and they are in a comatose or near-comatose state. Fortunately, hypercalcemic crisis is rare. Currently, the most common way patients find out that they have PHP is during a routine blood test or evaluation for low bone density (i.e. osteoporosis).
Over time, PHP damages almost every part of the body. Depending on how severe the disease is, PHP may cause virtually no symptoms or it may create severe, life-threatening symptoms. Doctors use the phrase "stones, bones, groans, psychic moans, and fatigue overtones" to remember that PHP can cause kidney stones, osteoporosis (i.e. weak bones), abdominal pain (i.e. pancreatitis, reflux disease), mental issues (i.e. depression, irritability, worsening concentration, worsening short-term memory, "brain fog"), and fatigue or low motivation levels among other things. When calcium levels become dangerously high (i.e. 13-15 range), patients may present in hypercalcemic crisis where their organs are failing and they are in a comatose or near-comatose state. Fortunately, hypercalcemic crisis is rare. Currently, the most common way patients find out that they have PHP is during a routine blood test or evaluation for low bone density (i.e. osteoporosis).
Osteoporosis
PTH signals the body to absorb more calcium from food and also to break down bone in order to raise the blood calcium levels. In PHP, the PTH level is constantly high so the body is constantly losing calcium from the bones. Eventually, the bones can become weaker and weaker and patients are more and more at risk for fractures (i.e. broken bones). The strength of a patient's bones can be measured with a simple test called a bone density scan. In this test, a specialized X-ray measures the bone density at the hip, femur (leg), spine, and forearm. The strength of the bone is compared to a healthy 30-year-old adult's bone density and given a score called the T score:
- Normal: T score between 0 and -1
- Osteopenia: T score between -1 and greater than -2.5
- Osteoporosis: T score less than or equal to -2.5
The lower the T score, the higher the risk of breaking bones. In an extreme form of PHP a bone disease known as osteitis fibrosa cystica can develop, in which the bones become so weak that they become soft and deformed. Fortunately, this is a very rare problem. Studies done at Columbia have shown that within a year of a successful parathyroid operation, patients usually gain about 10% of their bone density back and in addition stop losing their bone density at the faster rate caused by PHP.
Kidney Stones
High blood calcium levels can lead to high urine calcium levels. High urine calcium levels can cause stones to form in the kidney. These stones can be quite painful as they pass through the urinary system. They can also cause infections, blood in the urine, and kidney damage. Approximately 15% of patients with PHP will develop kidney stones. After a successful parathyroidectomy, the risk of forming new kidney stones returns to baseline (i.e. patients have the same risk as the average person).
"Non-specific symptoms"
 High calcium levels can affect every system in the body and lead to a variety of symptoms. These symptoms are often called "non-specific" because they can be caused by a number of different problems and are not specific or unique to PHP. In other words, just because a patient has parathyroid disease and these symptoms, it does not necessarily mean that their symptoms are caused by parathyroid disease or that these symptoms will get better after the parathyroid is removed. These symptoms may include:
High calcium levels can affect every system in the body and lead to a variety of symptoms. These symptoms are often called "non-specific" because they can be caused by a number of different problems and are not specific or unique to PHP. In other words, just because a patient has parathyroid disease and these symptoms, it does not necessarily mean that their symptoms are caused by parathyroid disease or that these symptoms will get better after the parathyroid is removed. These symptoms may include:
- Fatigue/Lack of energy
- Lack of motivation
- Muscle weakness
- Joint pain
- Muscle pain
- Bone pain
- Constipation
- Worsening concentration
- Worsening short term memory
- Slower information processing ("brain fog")
- Depression
- Irritability
- Anxiety
- Hallucinations
- Insomnia
- Worsening quality of life
Cardiac disease and shorter life expectancy
PHP may cause a number of problems with the heart and blood vessels that include hypertension (i.e. high blood pressure), coronary artery disease, atherosclerosis (i.e. hardening of the arteries), arrhythmias (i.e. abnormal heart rate), and left ventricular hypertrophy (i.e. enlarging of the heart). In turn these problems can lead to a higher rate of heart attack, stroke, and premature death.
Diagnosis
The diagnosis of PHP is made by measuring the blood calcium, PTH, and vitamin D levels. Normally, the calcium and PTH levels move in opposite directions of one another. See Overview ». In PHP, one or more of the parathyroid glands constantly make too much PTH causing an increase in calcium levels. In the majority of cases of PHP, the calcium and PTH are both high (i.e. above the normal range). However, in cases of normocalcemic PHP, the calcium may be normal even though the PTH is elevated. In some cases of PHP, the calcium level may be higher than the normal range and although the PTH is in the middle or upper end of the normal range, the PTH is inappropriately high for that calcium level (normally, as the calcium rises above the normal range, the PTH should fall below 20 or 30). Many experts believe that normocalcemic primary hyperparathyroidism is a mild form of classic primary hyperparathyroidism and that many patients will eventually develop classic PHP. This chart demonstrates the blood results for different types of PHP:
Blood Results for Different Types of PHP
- Condition: Classic PHP Calcium: High
PTH: High - Condition: Normocalcemic PHP Calcium: Higher end of normal range
PTH: High - Condition: PHP with inappropriately elevated PTH Calcium: Higher end of normal range
PTH: Higher than 20 to 30
It is important to check the vitamin D levels, because low vitamin D levels (i.e. vitamin D deficiency) can cause high PTH levels in a condition called secondary hyperparathyroidism. See Secondary Hyperparathyroidism ». In some cases, the 24 hour urine calcium levels should be checked to assess for the risk of kidney stones but also to rule out a rare condition called Benign Familial Hypocalciuric Hypercalcemia that does not require surgery. In this rare genetic condition, the blood calcium levels are high while the urine calcium levels are low.
Localization
 In 80% of cases of PHP, a single parathyroid gland is hyperactive (i.e. single adenoma) while the rest are normal. In 10% of cases, patients may have two (i.e. double adenoma) or three (i.e. triple adenoma) parathyroid glands that are abnormal, while another 10% have 4 abnormal glands (i.e. 4 gland hyperplasia). In some cases, surgeons perform a focused parathyroidectomy (See Focused Exploration »), in which they identify and remove just the abnormal parathyroid gland(s) seen on an imaging test. In other cases, surgeons perform bilateral neck explorations (See Bilateral Neck Exploration »), in which they look at all four parathyroid glands before removing the abnormal gland(s). Regardless of technique, it is critical to identify the abnormal parathyroid gland(s) before taking the patient to the operating room. Localizing tests are radiologic tests that are designed to identify the diseased parathyroid gland(s) and are often combined to improve their accuracy. Localizing tests include:
In 80% of cases of PHP, a single parathyroid gland is hyperactive (i.e. single adenoma) while the rest are normal. In 10% of cases, patients may have two (i.e. double adenoma) or three (i.e. triple adenoma) parathyroid glands that are abnormal, while another 10% have 4 abnormal glands (i.e. 4 gland hyperplasia). In some cases, surgeons perform a focused parathyroidectomy (See Focused Exploration »), in which they identify and remove just the abnormal parathyroid gland(s) seen on an imaging test. In other cases, surgeons perform bilateral neck explorations (See Bilateral Neck Exploration »), in which they look at all four parathyroid glands before removing the abnormal gland(s). Regardless of technique, it is critical to identify the abnormal parathyroid gland(s) before taking the patient to the operating room. Localizing tests are radiologic tests that are designed to identify the diseased parathyroid gland(s) and are often combined to improve their accuracy. Localizing tests include:
Ultrasound
 A non-invasive test that uses sound waves instead of radiation to create a picture. This test can often be done in the surgeon's office. This test is approximately 65% accurate in identifying abnormal parathyroid glands and the accuracy depends on the skill of the person performing the exam.
A non-invasive test that uses sound waves instead of radiation to create a picture. This test can often be done in the surgeon's office. This test is approximately 65% accurate in identifying abnormal parathyroid glands and the accuracy depends on the skill of the person performing the exam.
Sestamibi Scan (Nuclear Scan)
 A test in which a special radioactive tracer is given through the vein. The radioactive tracer is absorbed by the thyroid, abnormal parathyroid glands, and a few other organs like the heart. An additional advantage of sestamibi scan over ultrasound is that it can find abnormal parathyroid glands outside of the neck, for example, in the chest. This test is approximately 80 to 85% accurate in identifying abnormal parathyroid glands. In general, centers that perform a great deal of parathyroid surgery have more accurate scans.
A test in which a special radioactive tracer is given through the vein. The radioactive tracer is absorbed by the thyroid, abnormal parathyroid glands, and a few other organs like the heart. An additional advantage of sestamibi scan over ultrasound is that it can find abnormal parathyroid glands outside of the neck, for example, in the chest. This test is approximately 80 to 85% accurate in identifying abnormal parathyroid glands. In general, centers that perform a great deal of parathyroid surgery have more accurate scans.
High Resolution CAT Scan (Parathyroid series, 4D CAT Scan)
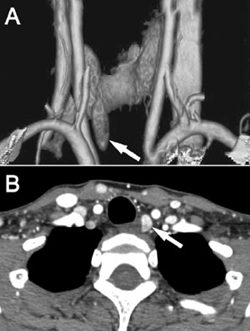 A special type of CAT scan that is done specifically to identify abnormal parathyroid glands (normal CAT scans are not very accurate at finding abnormal parathyroid glands). Whether or not a parathyroid is abnormal can be determined based on how quickly contrast (i.e. a dye that is given through the veins) washes in and out of parathyroid glands as well as the size of the parathyroid glands. This test is approximately 95% accurate in identifying abnormal parathyroid glands. This specialized test is only available at select institutions.
A special type of CAT scan that is done specifically to identify abnormal parathyroid glands (normal CAT scans are not very accurate at finding abnormal parathyroid glands). Whether or not a parathyroid is abnormal can be determined based on how quickly contrast (i.e. a dye that is given through the veins) washes in and out of parathyroid glands as well as the size of the parathyroid glands. This test is approximately 95% accurate in identifying abnormal parathyroid glands. This specialized test is only available at select institutions.
MRI
Is not very good at identifying abnormal parathyroid glands and is therefore not routinely used. In cases where ultrasound, sestamibi, and high resolution CAT scan are negative or in re-operative parathyroid surgery, MRI may occasionally be used.
Parathyroid Fine Needle Biopsy
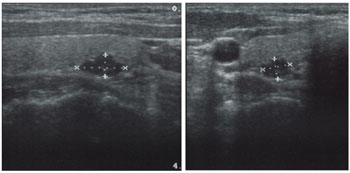
A test in which a nodule that is suspicious for an abnormal parathyroid gland may be biopsied using a small needle under ultrasound guidance. The biopsy analysis includes looking at the cells to see if they look like parathyroid cells as well as measuring the PTH level in the sample. This test is not performed routinely and is usually only used if there is a question of whether or not a nodule is an abnormal parathyroid gland or something else like a thyroid nodule or an enlarged lymph node.
Ultrasound guided fine needle biopsy demonstrating the needle (white line) sampling the nodule
Selective Venous Sampling
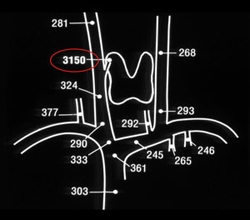 A special test in which a physician places a catheter into the large vein in the groin and then measures PTH levels from blood samples drawn directly from the veins that carry blood away from the parathyroid glands. Selective venous sampling is usually done in cases where ultrasound, sestamibi, and high resolution CAT scan are negative or in re-operative parathyroid surgery. This test is only available at select institutions and is usually performed by a vascular surgeon or interventional radiologist as an outpatient procedure.
A special test in which a physician places a catheter into the large vein in the groin and then measures PTH levels from blood samples drawn directly from the veins that carry blood away from the parathyroid glands. Selective venous sampling is usually done in cases where ultrasound, sestamibi, and high resolution CAT scan are negative or in re-operative parathyroid surgery. This test is only available at select institutions and is usually performed by a vascular surgeon or interventional radiologist as an outpatient procedure.
Combining the results of these tests may improve the accuracy of localizing the abnormal parathyroid gland(s). For example, if an ultrasound and sestamibi scan agree as to the location of an abnormal parathyroid gland, there is an approximately 96% chance that it is the only diseased parathyroid gland. Since the accuracy of these tests can vary from place to place, it is critical to work with doctors who are experts in parathyroid disease in order to decide which localizing tests are needed.
Treatment
Parathyroidectomy (i.e. surgical removal of the parathyroid gland) is the only known cure for PHP and is often the best treatment for this disease. In the hands of an experienced surgeon, parathyroidectomy will cure up to 98% of patients with this disease. Alternatives to surgery include observation and medical therapy. Patients who choose observation may have progressive worsening of their disease over time leading to an increased risk of kidney stones and osteoporosis. Most of the best medical therapy available is aimed at treating the symptoms of the disease rather than curing it. For example estrogen and bisphosphonates can improve or maintain bone density but will not fix the underlying problem. A group of medications called calcimimetics (ex. Sensipar, Cinacalcet) "trick" the body into lowering the blood calcium level. However, calcimimetics will not cure the parathyroid disease and they do not seem to lower the risk of kidney stones or help protect bone strength. While surgical therapy is the best treatment for PHP, medical therapy may be chosen for patients who have medical problems that make them high-risk candidates for surgery.
When determining which patients should have parathyroid surgery, the National Institutes of Health (NIH) groups patients into two categories: symptomatic and asymptomatic. The NIH considers patients who have kidney stones, osteitis fibrosa cystica, and/or hypercalcemic crisis (i.e. very high calcium levels causing organ failure and potentially coma) as having symptomatic disease. Patients with symptomatic PHP should have a parathyroidectomy if at all possible. The NIH considers all other patients with PHP as having asymptomatic disease. This group includes patients with the non-specific symptoms of parathyroid disease. For patients with asymptomatic disease, the NIH guidelines state that patients should have a parathyroidectomy if they have one or more of the following:
- Blood calcium level greater than 1mg/dl above normal
- Glomerular filtration rate (i.e. kidney function) less than 60 ml/min
- Osteoporosis (i.e. T score less than -2.5) or previous fracture
- Age less than 50
- 24 hour urine calcium level greater than 400mg/24 hours (current guidelines do not include this condition, but some experts still use it)
While these guidelines are useful, many parathyroid experts feel that there are more patients with PHP who would benefit from an operation. In fact, many patients with asymptomatic disease will get worse and worse over time and may benefit from an earlier operation to avoid the complications of parathyroid disease. For this reason, it is critical to consult with an expert in parathyroid disease to determine which patients should have an operation.
Next Steps
If you are dealing with a parathyroid issue, our team at the Columbia Parathyroid Center is here to help. Call (212) 305-0444 or request an appointment online.