Key Takeaways:
- Recent updates to lung cancer screening criteria that lower age and smoking history thresholds aim to significantly increase the number of eligible individuals, potentially saving more lives.
- Despite proven mortality reduction, lung cancer screening faces hurdles like false positives and historical stigma, yet the National Lung Cancer Screening Trial demonstrated unparalleled effectiveness, underscoring the urgent need for broader adoption.
- With lung cancer becoming more prevalent among non-smoking women and BIPOC individuals, efforts to improve screening access and coverage must address disparities, emphasizing education, infrastructure, and insurance reimbursement to ensure equitable care.
A conversation with Bryan P. Stanifer, MD, thoracic surgeon and Director of the Women’s Lung and Health Center at Columbia, about the most recent change in lung cancer screening guidelines.
Talk to us about the new lung screening guidelines. What’s changed?
The two biggest changes were dropping the age criteria and the amount of smoking you have to have done in the past. The criteria went from age 55 to 50 and then from 30 pack years to 20. So that will dramatically increase the number of people who should get screened.
And 20 pack-years is honestly what we use already, even in lung transplant.
What does the term “pack years” mean exactly?
It’s actually a calculation—packs per day divided by the number of years. You can get there many different ways, all different iterations. People smoking three or four packs a day get there much, much quicker. It doesn't just mean you smoked a pack a day for 20 years.
Who’s on this advisory panel, the U.S. Preventive Services Task Force?
It's a government-based panel. These bodies are systematic data-driven panels that look at what the actual evidence is and then factor in costs and benefit in a way that's a little unusual. I'll be honest with you, it's surprising that they did this.
The history of The National Lung Cancer Screening Trial was a massive multi-year, I think a hundred+ million-dollar trial that the NIH funded originally, which showed that low dose lung cancer screening not only decreases lung cancer-related mortality by 20 percent but decreased all-cause mortality by almost 7 percent. You can go through and look at screening programs for virtually everything else in medicine. This blows them all out of the water.
In terms of mortality benefit, major mortality, there's nothing else like this, whether it's breast cancer screening, prostate cancer screening, cervical cancer screening, it's far and away, the biggest benefit ever shown for any screening program. Even with that, it almost didn't get approved by the U.S. Preventative Services Task Force.
Why is that?
There are a lot of false positives. So, they start looking at different screening metrics: number needed to treat to benefit/number needed to treat to harm. The false narrative numbers are big. We all have lung nodules just from environmental exposure, maybe you had an asymptomatic infection. There are many different things that can cause lung nodules.
So, there was a huge push by the Society of Thoracic Surgeons and pulmonologist societies, and there was a lot of confusion at first because all these different societies came out with different criteria. Looking at different age ranges, different smoking pack-year ranges. But finally, after all this lobbying, it got approved. The big issue is that the insurances didn't adopt it. So right now, today, we don't even have a lung cancer screening program at Columbia. That will soon change.
Wow. Because no insurance has covered lung screening up until this point?
Yes, because the economics are so poor. With anything in medicine, the filtration of the knowledge of the benefit is slow, and then the economics of what insurances are willing to pay for it is quite poor.
So, barrier to access is a major issue here.
Huge barrier. Even major institutions like ours still don't have a lung cancer screening program. But we are now finally opening one, I've taken over that effort. We're opening up the site in Tarrytown this year.
Will you break down the details of this lung cancer screening trial? What’s the bottom line?
Screenings give a 20 percent benefit for lung cancer mortality, basically 7 percent benefit all-cause mortality. When you start scanning people's chests, you find other things, you find problems with their heart, problems with their aorta, problems with their chest wall, or even breast cancers can be found with a CT scan. This is a huge benefit.
It isn't the only trial that looked at this either. There's one from Europe called the Nelson trial, which was really mostly focused on men—and mostly white men—but it did include about 2,500 or so patients who were women and showed an even greater survival advantage.
What was the difference in survival advantage between these trials?
In the Nelson trial, the rate of death in men in the screened group at 10 years was 0.76, basically a 24 percent survival advantage. If you look at the subset of women who were included in the trial, which wasn't powered and designed for women, it’s 0.67. You're getting over 30 percent survival benefit if you're a woman who's being screened.
Now the caveat is that numbers were small, only 2000 patients, and it didn't meet statistical significance. But the trend was so clear that if you bump those numbers up to 5,000 patients, you unquestionably would have had statistically significant improvement in the women too. So, it's a huge benefit.
Are there more studies now focusing on women and BIPOC patients specifically? The recent New York Times article states that Black Americans and women tend to develop lung cancer earlier and from less tobacco exposure than white men.
The data here is a little strange because in the background of the screening update there's been data looking at who's getting increased lung cancers now in the United States. And it's actually mostly not the Black population, it's the Hispanic population and the white population. The rates of smoking across races aren't dramatically different based on the most recent data that I've seen, probably from some time in the mid-2010s.
There are a couple of messages here—lung cancer is the number one killer for everybody, period. Whether you're a man, woman, Black, white, Hispanic, you've got to add the next five or six cancers together to get to the same yearly deaths that we get from lung cancer.
What we do know is that lung cancer is increasing in women. That's been shown in another NEJM paper we did a big push on around 2018. That same paper also showed that most of it is being driven again by non-Hispanic whites and Hispanics generally. I don't have much to tell you about the Black or African-American population, because the data just hasn't panned out yet. I know the New York Times is saying it, but in terms of data, I can't point to a study.
Interesting. What about factors beyond smoking, secondhand or passive smoking, are those risk factors included in the annual screenings criteria?
Secondhand smoke is never going to qualify based on these criteria, this is actual smoking. There are clearly patient populations that are going to not fall into this, and specifically, it's the young non-smoking women who still aren't going to be included in this, who are making up an increasing percentage of the patients that we see.
And a whole 15 percent of lung cancers, non-small cell lung cancers, develop in non-smokers. Two-thirds of them are women.
Wow. Why aren’t there screening criteria for non-smokers? It’s shocking to hear when you explain these numbers.
Well, the history of screening for lung cancer before the advent of CT scans was all done by chest x-ray. And to see a lung cancer on a chest x-ray, they've got to be pretty big. They looked at this back in the 80s and 90s, and there was no benefit because you were only finding tumors that probably had an average size of five centimeters.
Once your lung cancer is five centimeters, you're pretty far along. With CT scans, you're finding one, two, three-centimeter tumors. Those are people who probably don't have nodal disease and who could be potentially cured with surgery.
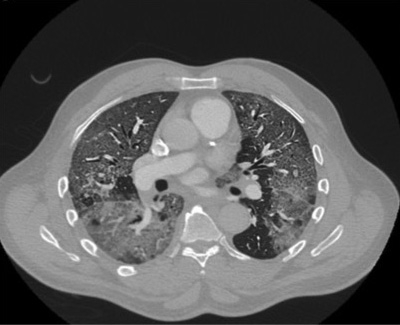
What are you looking for on a CT scan, and what’s the screening like for a patient, the process and experience?
Well, if you fit the criteria based on age and smoking history, you're sent for what's called a low-dose CT scan. You're getting less radiation, which probably has some small benefit. And we’re looking for lung nodules. Lung nodules come in three flavors; solid, Ground Glass Opacities (GGO), and mixed nodules.
Solid nodules we worry about the most. You've got a two-centimeter solid lung nodule, something needs to be done. You need a diagnosis, biopsy, surgery. What we call GGO or Ground Glass Opacities are a little bit harder to deal with and still need to be followed. They can be potential lung cancers, but it’s less clear. And then there are these mixed nodules that are mostly ground-glass but have a solid component. Those are also concerning for developing lung cancer.
If you fit the criteria, should you be getting an annual screening indefinitely or is the recommendation for a fixed period of time?
Well, I'll tell you my opinion. If you're continuing to smoke, you need ongoing screening. The risk for developing lung cancer doesn’t really ever go to zero if you smoke for 30 years.
The way we do this is based on nodule size and nodule characteristics. There's something also out there called the Fleischer criteria, which we all use to help provide some general guidelines. And the magic number for lung nodules is one centimeter. Things that are one centimeter either need a diagnosis, need to be closely followed, or you need to go to surgery for both the diagnosis and treatment at the same time, depending on the situation. The size, the actual characteristics of the nodule—the terminology we use is spiculated, meaning they have an irregular border. Those are very concerning for a lung cancer.
Walk us through the process of getting screened and having a nodule found on the CT scan.
Here’s a typical example. If you've got a seven-millimeter solid nodule we would probably say we need to see you in three to six months with another CT scan, even sooner than one-year. Let's say that thing has now grown to a centimeter, well, something needs to be done. We need to figure this out.
Or we scan you again in three to six months and we find it's still seven millimeters. So, let's say we did three months to start. All right, next, you come back in six months, it's still seven millimeters. Okay, come back in a year. When there are no changes we sort of lengthen the time in between screenings. We're looking for prolonged, increasing periods of stability to indicate that it's probably not a lung cancer based on its behavior.
Could you have symptoms with smaller nodules?
Most are asymptomatic, the vast overwhelming majority. It’s very rare to have symptoms with something that small. Every now and then you'll have one that's in a weird location and somebody may be able to cough up blood, or if it's very close to an airway they may have a chronic cough. Those are two red flags symptoms and you need to come in for CT scan imaging to rule out a problem, like a lung cancer.
How can we improve access to lung cancer screening? What would you like to see?
Like with any screening program, first of all, there's the education component. And it's the education of both the patient and the primary care provider, but also general pulmonologists.
We need programs and structures in place because there are going to be a lot of false positives. So, you need to have a structure to deal with that—to track and follow those patients over time. For us internally, we just need the actual infrastructure in place, in terms of people to run the program. For the referring provider’s portion of this, it's opening up the knowledge and convenience of getting the CT scan.
And payers, insurances, should really be reimbursing for this. The benefit is huge and it's been repeated now in multiple large trials. 53,000 patients were in the national lung cancer screening trial. 53,000.
It’s a bit bewildering to hear you explain the data, the immense benefit of screening, yet lung cancer screening is not universal and still isn’t covered by most insurance. Meanwhile, breast cancer, ovarian cancer screening is. Why? As the kids say, make it make sense.
There are two components to this. Lung cancer historically has had a stigma. It was mostly, you know, angry old men in their seventies who smoked. Nobody really cared about them. “They did it to themselves, blah, blah, blah.”
The other component is there's been nobody advocating for it. The great example of cancer advocacy is obviously breast cancer. The Komen Foundation and on down, those groups have strongly advocated for their patients. It's the most frequent cancer in women, but the reality is most women aren't dying of it, right? It's not even close to the number of women who are dying of lung cancer. It’s an order of magnitude less.
Over time I think we're doing better on the advocacy front. Also, the demographics are changing. You've got all these 45-year-old, never-smoking women now who present with stage four lung cancer. That's a lot more sympathetic, it’s just the reality of how the world works. So, it is increasingly appreciated. And these massive trials have just proven what we all thought was true.
If you were able to screen everyone who fits these criteria—everyone you would want to screen—how would lung cancer survival and mortality change? How much of a benefit would you expect?
Well, the more people you screen the less benefit you're going to see. The reason the screening criteria were what they were is that they were trying to increase what’s called the pre-test probability.
If I take the highest risk group, the likelihood that before a test they're going to have a positive screen is much higher. But if I screen all the non-smoking women between the ages of 40 and 50, I'm going to have very few positive tests. So, the benefit of screening is going to go down.
But if we were to screen everybody who smoked greater than, let's say 15 pack-years and drop the age criteria to 45? We probably would drop the mortality benefit to maybe 15 percent, and 5 percent all-cause mortality.
The problem is that lung cancer is so deadly. You're still looking at five-year survivals of 20 percent. So, that's the reason for trying to aggressively screen as many people as possible.
What we really need to do is identify the non-smoking cohort and figure out who these people are. You've heard of the BRCA gene change for breast cancer—is there some yet unidentified equivalent for that in these lung cancer patients?
Are there any leads on that front in genetic research?
What we know is that about 40 percent of them have something called an EGFR mutation, which is the cause of their lung cancer. And if they have that mutation, that's great because there are lots of targeted therapies for those patients that are much more effective and less toxic than traditional and radiation.
60 percent of them though we have no idea. And what I've wanted to do since I came here was get a study up, looking at those patients. With Covid and everything else we haven't yet done it, but that's the goal.
Do you find there is new attention being paid to lung cancer because of Covid? The research and treatment of long-term effects, the many unknowns—could this be a big push for your efforts?
Oh, no doubt. Covid has put lung disease back on the map. Whether it's mostly through the lens of lung failure, lung transplant, and ECMO [Extracorporeal Membrane Oxygenation]. But most people aren't going to need a lung transplant; most people aren't going to need ECMO.
We are going to have patients with chronic long-term lung disease from Covid. I think some of those patients are going to have a form of, or they may already have a form of interstitial lung disease.
Who is at risk for interstitial lung disease, Covid aside?
We wish we knew that, too. Interstitial lung disease is kind of a broad category that includes lots of different things. And some of them have an identifiable cause. For example, there's something called hypersensitivity pneumonitis that's related to environmental exposures. Classic examples: people who have exposure to a lot of dust in an industrial or agricultural setting, a lot of hay exposure. People who keep birds also get it.
But then most of it is idiopathic, meaning, we don't know why they get it. The classic example is called IPF, idiopathic pulmonary fibrosis. Huge lung cancer risk, much worse than COPD. And those patients develop fibrotic lungs that are also seen on a CT scan. So that crowd definitely needs to be screened for lung cancer because the risk is really significant. You don't have to have been a smoker to get interstitial lung disease.
What’s the most important thing you want us to take away from this update to screening guidelines?
The change is very good. If you qualify, you really need to go get the screen. It's totally non-invasive, the actual scan only takes a few minutes. It's not one of those claustrophobic MRI things. It's fast, there's a huge benefit. And again, not just for lung cancer mortality, but for all-cause mortality.
And for those who fit the criteria, it should now be covered by insurance—because of this change. Generally speaking, when a governing body makes these changes or recommendations, Medicaid covers it. And it’s expected that all the other insurances will as well. That’s the norm. Lung cancer screening works, and we need it more broadly. Most importantly, we need you to get involved—bring it up to your primary care doctor or pulmonologist. Screening saves lives.
Click here to learn more about lung diseases and treatments. To schedule an appointment with a specialist at the Surgical Lung & Chest Care program please call (212) 304-7535.
Related:
- State of the Union: Lung and Chest Care
- Advancements in Immunotherapy a Huge Boon for Lung Cancer Treatment
- I Love The Skin I Am In—Life After Nuss Procedure for Chest Deformity