Updated November 2024 by Dr. Roshni Rao.
An interview with Roshni Rao, MD, Chief of the Division of Breast Surgery.
What's new in breast care? Have we seen breakthroughs in any area?
It’s the management of patients post-operatively where things are changing most. We're really trying to minimize our use of opioids, especially for breast patients, by using what we call multi-modality approaches. We're not only infiltrating things during the operation. We're giving them blocks by anesthesia beforehand; we're setting them up to get a few medications in the post-op setting, including standard ones like Tylenol, Advil, as well as nerve medications that we put them on for seven to 10 days. We also use ice a lot, even aromatherapy. And we're putting all these things together so that we can avoid narcotics. So, we have a nice pathway we've developed here that we try to put patients on routinely, and it’s been really helpful in reducing our use of them.
Can you explain that pathway a little bit more? What can patients expect?
I think the key thing is that we understand surgery can be painful for some patients. It's definitely not that we don't acknowledge that. It's just that for the majority of patients, especially with the types of operations that we do, narcotics are not really necessary. Or we can minimize using them as much as possible so we will give you other methods for relief and pain control. With this approach, we're trying to figure out any other way to get these patients through their post-op recovery very comfortably, but without a narcotic.
When we first spoke about this in 2020, you had just released a paper on post-op pain management. It’s pretty remarkable to see the success of these multi-modality approaches from the patient's perspective.
Right, right, it is! I think there is this thought process that if you have surgery, “make sure they give you a pain medication.” And in most of our experiences, with a lot of our patients, they feel like they need to take it because we're giving them this prescription. Then they end up taking one or two. And what do you do with the rest of them? That’s one of our concerns. If you look online like I was, I saw this complicated approach to properly get rid of narcotic medications. You have to get coffee grounds and ground it...And it's a whole crazy thing.
Is there anything else we should know about the pain management studies you’re doing?
The trial is still ongoing, and it's done in conjunction with our medical oncology group, led by Dr. Dawn Hershman. This trial uses a prescription bottle that is connected to an app on your phone. When patients are scheduled for surgery, and we prescribe some number of medications, they get the app, and this bottle of medication is mailed to them.
And let's say they're starting to have some discomfort; they click on their app. It asks them some questions about their pain level. Based on that, it tells you, “Oh, why don't you try a Tylenol?” Or it says, “Oh yes, you probably need a narcotic.” And then, it gives you a code to open up your narcotic bottle. When you're done after 10 days or so, whatever you haven't used is mailed back in the bottle. It's a whole concept of avoiding these pills continuing to circulate randomly.
Let’s talk about some of the newer aspects of surgery. What advances are you seeing?
One of the biggest things we’re doing in surgery is moving toward a more multidisciplinary or even transdisciplinary approach. It used to be that some problems were purely surgical, but now most medical conditions are multifaceted. No surgeon works in isolation—whether it’s cardiac, vascular, or breast surgery. We work alongside our colleagues from other specialties because the patient’s treatment plan is a team effort. For example, in breast surgery, we work with oncologists, geneticists, and radiologists to determine the best approach for each individual case.
What about surgical approaches? Have there been any recent changes or updates?
The first is that we’re still offering intra-operative radiation therapy for certain patients, and now we have long-term data on it. There's always been a question when we do intraoperative radiation therapy: “Is it really enough long-term?” And we've found through the Target Trial that it is enough for the long term.
When is intraoperative radiation used? What types of cancer?
It's only for very selective patients. Generally, we say they have to be at least 50 years old and not have particularly aggressive cancers. It has to be less than three centimeters and can't be in the lymph nodes because intraoperative radiation is very, very focused and targeted. So, it has very specific criteria. If you have cancer in your lymph nodes, that area also needs to receive some radiation, and this is not sufficient.
What’s recovery like for someone getting radiation intraoperatively?
It’s much easier. Standard radiation involves coming in five days a week for three to six weeks. You can imagine having to be somewhere five days a week for three weeks and that potential exposure to sick people during transit and those types of things. I think it's very helpful for a lot of our patients to know that they're going to come in once, get their lumpectomy, get the radiation, and they’re done.
Has anything changed in terms of your approach to mastectomy?
The I-SPY trials are really starting to change how we think about surgical approaches. The adaptive model allows us to evaluate experimental agents and treatments we give before surgery in an efficient way that moves quickly. One of the studies we published recently looked at removing fewer lymph nodes by placing a clip in the node before surgery, which helps us target just the affected node during surgery. This de-escalation of axillary surgery is significant because it helps reduce the risk of lymphedema, nerve damage, and arm swelling, which can happen when too many lymph nodes are removed.
Additionally, I-SPY is looking into the role of radiation after lymph node involvement. Traditionally, patients with cancer in their lymph nodes automatically received radiation. Now, we're seeing that if the cancer responds well to treatment and is no longer present in the lymph nodes by the time of surgery, some patients may not need radiation at all. That's an exciting area we’re working on.
What should patients know about lymphedema after surgery?
Lymphedema remains a concern, especially for patients who undergo complete lymph node dissection. The risk for those patients is about 30 percent, while for patients who only undergo a sentinel node biopsy, it’s around 1 percent. So, it’s a much bigger issue for patients who have all of their lymph nodes removed. But we're taking steps to reduce that risk, especially with the I-SPY trial and other de-escalation approaches in axillary surgery. One of the most exciting developments is a national trial on axillary reverse mapping, led by Dr. Bret Taback, which is focused on preserving lymphatics during surgery to potentially prevent lymphedema.
Are there any updates on nipple-sparing mastectomy?
Yes, we’re offering more and more nipple-sparing mastectomies. The ideal candidate for this is someone whose cancer is small, not near the nipple, and whose nipple is in a very youthful position. Having said that, we are able to, if a patient is very motivated for nipple-sparing, sometimes in conjunction with our plastic surgery colleagues, we're able to do a reduction upfront and then do a mastectomy later on and be able to save the nipple.
What other changes in breast cancer treatment should patients know about?
I mentioned the I-SPY trial earlier, and it continues to evolve. We're seeing new insights around genetic testing and personalized treatment approaches. For example, we’re now routinely offering genetic testing to patients under the age of 65, compared to the older, more limited criteria. And although it’s an area of controversy, there's a move to offer genetic testing to every breast cancer patient. This is largely because genetic testing has become less expensive and more accessible.
However, one challenge is that sometimes we find gene variants that don’t mean anything, which can cause unnecessary anxiety. This is an area where the field is still divided. Some experts argue for universal genetic testing, while others believe we should remain selective. It ultimately comes down to a conversation between the physician and patient to determine what’s best for each individual.
Anything new with medications and immunotherapy to be aware of?
One of the most exciting medication areas right now is CDK 4/6 inhibitors. These are treatments for hormone receptor-positive patients, and they’re becoming a major tool in preventing cancer recurrence for certain select patients. It’s a pill they take for two to three years, and the data supporting its efficacy continues to grow.
Another important development is the Breast Cancer Index (BCI), which helps us determine whether patients might benefit from extending their hormonal treatment—like tamoxifen or anastrozole—from five years to 10. We do additional genetic testing on the tumor itself to help figure this out. This is an area of ongoing research, but it’s a significant step forward in understanding which patients may need longer-term treatment.
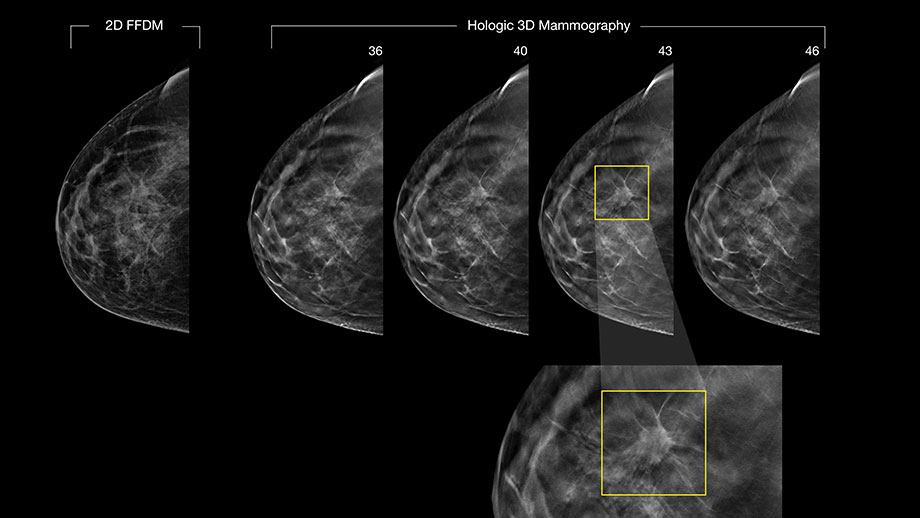
Let’s pivot to preventative care. What’s the latest on 3D mammograms? Are they now recommended for all patients?
Yes, absolutely. We recommend 3D mammograms for everyone. The good news is that 3D mammography has become the standard at all of our centers, and it does make a difference, especially for patients with dense breast tissue. 3D mammography allows us to see more of the dimension of the tissue, and it picks up more cancers in dense breast tissue than traditional 2D mammograms. I think it’s very helpful for all patients.
Recently, a Yale study confirmed that 3D mammography is superior to 2D, and we're seeing most insurances in New York now covering it. This is great news because patients no longer have to pay extra for 3D mammograms, which used to be an additional out-of-pocket cost.
It also reduces the rate of false positives. In the past, we’d often see something on a 2D mammogram that required more follow-up work or testing, but many times it turned out to be nothing. With 3D mammography, we’re getting more accurate results upfront, so there’s less unnecessary anxiety and fewer follow-up appointments for patients.
What do you think breast care will look like in, say, 10 years?
I think the exciting thing is that it will be more and more individualized. That’s where everything is going, trying to really sort out exactly what this treatment needs versus that treatment. This tumor versus that tumor. I think that's really where it needs to go. And that’s where our collaboration is headed.
Fortunately for us, the entire care team is on the same floor. So, we have our medical oncologist, radiologist, and surgeons all on the same floor. We're not in different buildings; we're all right here. We have a very close relationship, and we're constantly texting each other through Epic [the medical records system] about our patients. We have meetings every single week, at least once a week. Many times, two or three times a week, to discuss things. It works really well and strengthens that individualized approach, and certainly, collaboration will continue to strengthen and expand in the future.
Related:
- For Many Breast Cancers, There Is No Advantage to Mastectomy
- New Breast Cancer Guidelines Say Mammograms Should Start at Age 40
- Advancing Breast Cancer Treatment: Dr. Roshni Rao on the Latest Breakthroughs from the I-SPY Trial